Anesthesia/Sedation
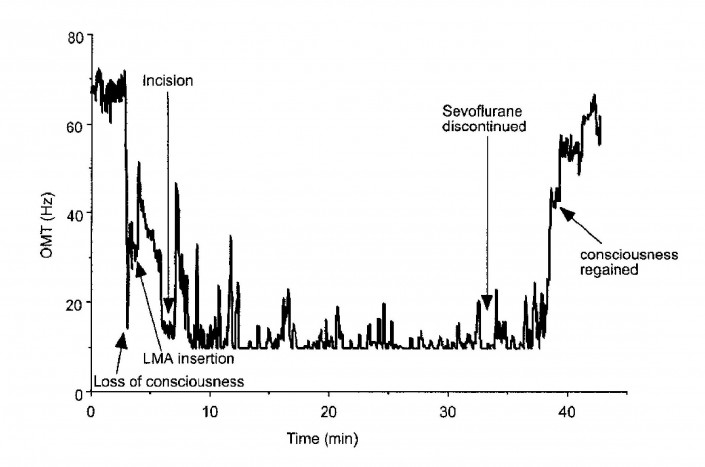
Clinical research has shown that OMT activity decreases in response to anesthetics and sedatives. OMT has been shown to provides a clinically meaningful measure of sedation level. Monitoring of the OMT frequency during anesthesia and sedation may help clinicians target the ideal dose and sedation level for individual patients.
Critical Care Sedation
Today approximately 80% of patients in the ICU receive sedatives to manage anxiety, agitation and provide hypnosis. However, many patients are not monitored for their clinical level of sedation; clinicians often rely on subjective impressions of a patient’s level of sedation. Despite the known benefits and wide acceptance of administering drugs flexibly to achieve target sedation level goals (as opposed to administering drugs based on constant volume rates), this practice is difficult to achieve without a realtime, reliable and objective measure of a patient’s true level of sedation. (Jackson, 15)
Other subjective scales of sedation are sometimes used in the ICU. Although these measures are valuable for assessing patient agitation, none were created for the purpose of measuring depth of anesthesia and do not provide the sensitivity and specificity required to truly manage sedation. (Kevin, 8)
 The SCCM does not recommend that Bispectral Index [BIS] be used as the primary method to monitor depth of sedation in non-comatose, non-paralyzed critically ill adult patients. – 2012 Practice Guidelines
The SCCM does not recommend that Bispectral Index [BIS] be used as the primary method to monitor depth of sedation in non-comatose, non-paralyzed critically ill adult patients. – 2012 Practice Guidelines
OMT and Depth of Anesthesia
A multi-center study of 214 patients illustrated the ability of OMT to accurately discriminate between asleep and awakened states of consciousness. OMT frequency was used to predict a subject’s ability to respond to verbal command following emergence from anesthesia. Statistical analysis showed high sensitivity and specificity of OMT as a predictor of return to consciousness in surgery patients. (Heaney, 7)
Ineffective Alternatives Today
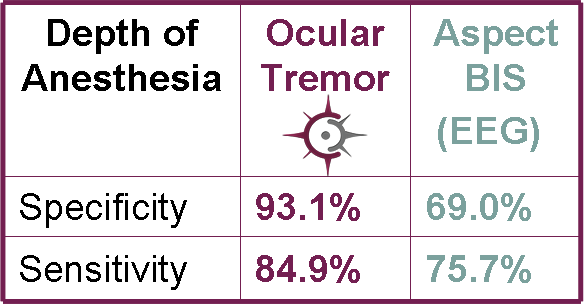
Objective measures remain elusive in the determining depth of anesthesia and sedation. A number of clinical monitors have made their way into the market, but none have been universally adopted by clinicians. A published comparison of bispectral index (BIS), an EEG based method of monitoring sedation, showed that OMT was more sensitive and specific in distinguishing awake vs. anesthetized state. In addition, BIS showed increasing variability at deeper levels of sedation. (Kevin, 8)
“Just last week I really needed this on two of my patients.”--Joseph Varon, MD, Chief of Staff and Chief Critical Care Services University General Hospital and Professor, The University of Texas
Neurodiagnostics
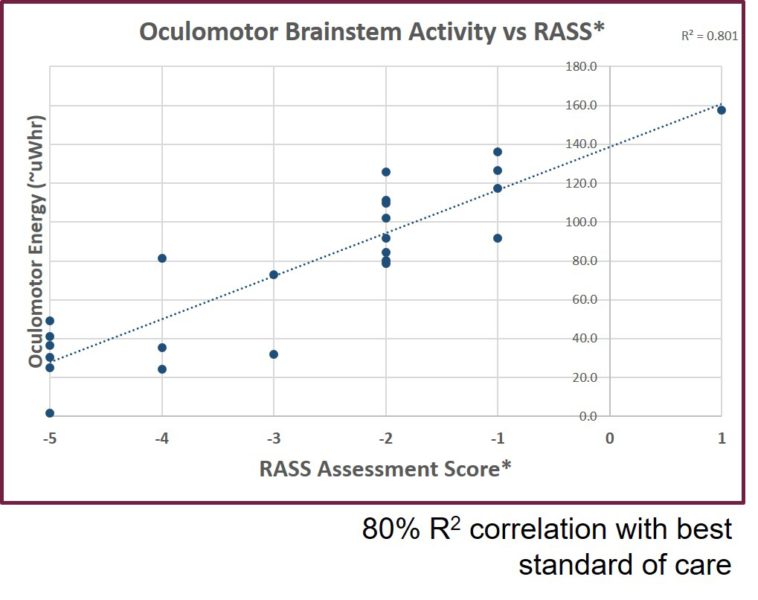
Measuring OMT frequency has a number of useful applications in the clinical setting. Decreased OMT frequency shows strong correlations as a diagnostic for conditions that affect the oculomotor neurons leading to the brainstem and the brainstem itself.
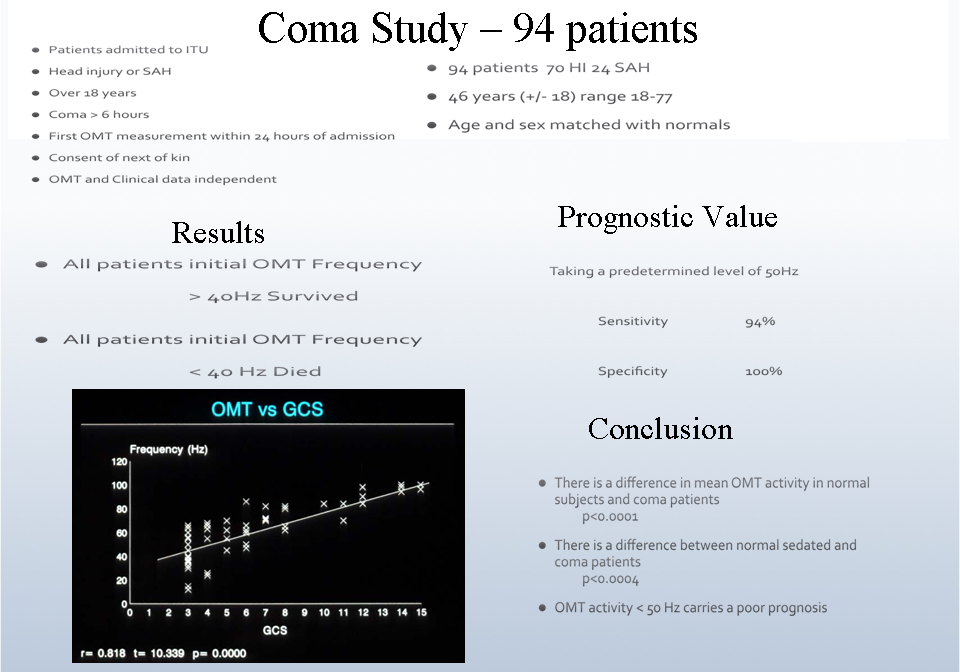
Coma Prognosis
Several studies have confirmed the prognostic value of OMT for coma patients. Low OMT frequency at admission to the hospital in comatose patients is a strong predictor of early death. In a study of 32 patients, OMT frequency of <50 Hz was associated with early death (sensitivity=1.0, specificity=1.0, PPV=1.0, NPV=1.0). All patients who presented with an initial OMT frequency of >50 Hz regained consciousness. (Bojanic, 37) A coma study including 94 patients showed similar results (Bolger, 38):
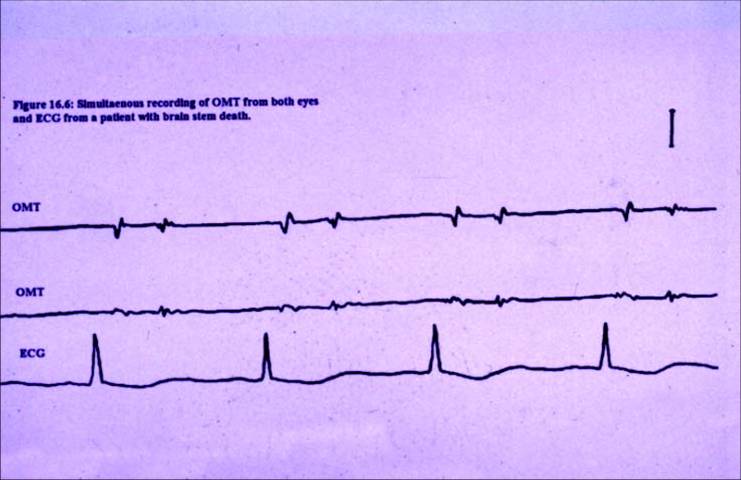
Brainstem Death
Assessing brainstem death is another challenging area for clinicians as there is no truly objective diagnostic method available. Brainstem death is diagnosed using a series of neurological tests administered by more than one clinician and is generally confirmed by EEG. A clinical study of 42 patients concluded that OMT activity is a sensitive and objective method of detecting brain death. Of the 42 patients, 39 were determined to have brainstem death by current clinical standards. Thirty-eight of the 39 showed no OMT activity. (Bolger, 39)
Parkinson’s Disease
There is no definitive diagnostic test for Parkinson’s Disease. Diagnosis is made clinically based once the patient becomes symptomatic. Brain scans may be used to rule out other conditions, but cannot detect Parkinson’s specifically. Patients are often misdiagnosed (up to 15% of the time) and it is recommended that the diagnosis be reviewed throughout the patient’s treatment.
Patients with Parkinson’s disease differ significantly from normal healthy subjects on multiple features of OMT activity including overall frequency (Hz). The Brainstem Biometrics TMU may have clinical use not only as an early marker for Parkinson’s disease in individuals, but may also be useful in guiding treatment. (Bolger, 35)
Multiple Sclerosis
Multiple Sclerosis (MS) is a manifestation of lesions which occur in the central nervous system due to an autoimmune response on the myelin sheath of nerve cells. Diagnosis can be difficult and requires serial brain MRI testing not only for diagnosis, but to monitor the progression of the disease. Different subgroups of MS patients with and without brainstem or cerebellar disease have shown different mean OMT frequencies relative to each other and to control patients. The use of OMT in this patient population may provide insight into disease staging and treatment response. (Bolger, 36)